 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv Today in Washington CSPAN March 19, 2013 6:00am-9:00am EDT

























































6:59 am

>> our proposal in october 2011 said it. and strain on the number, maximize that gap by cutting specialty fees while holding primary-care constant. if you have more money available though, it would obviously be desirable to increase primary
7:00 am

care. >> thank you, mr. chairman. >> mr. smith. >> thank you, mr. chairman, and thank you, mr. hackbarth, for sharing your perspective and insight on some very important issues today. it's my understanding and i think this topic was touched on briefly but there are various factors that perhaps leading to more and more provider consolidation. could you elaborate more on that? and perhaps share what you see on the impact to insurance premiums as a result of? >> i would say there are basically two. one, there is consolidation. that is aimed at developing new organizations that are better able to effectively care for medicare patients and other patients your so they are integrating in the way that they collaborate, to better coordinate and integrate care. that's the type. then there's the other type that is basically aimed at maximizing
7:01 am

market power. and so there have been a lot of what antitrust lawyers would refer to as horizontal mergers where hospitals are joined together, not integrating with physicians, just building hospital systems that have more leverage, vis-à-vis insurance companies. that's more problematic. the tricky part is some of the good type of integration also leads to market power that can lead to higher prices for private parties. >> and i can appreciate a lot of things about how different health care is delivered, how differently health care is delivered across the country. certainly represent a very rural area, and i think there's still some consolidation out there, for various reasons. so i appreciate that. now shifting gears a bit. in terms of reimbursement, and i
7:02 am

noticed the commission has recommended steps that medicare can take to make sure it is paying accurately for each individual physician service. and without getting into the details too much here, why would you say it's important that he determination is accurate and one of the implications perhaps for getting them wrong? >> there are two types. the one we just touched a minute ago. if the prices are wrong again influence the physician pipeline fofor the future. sewickley consistently underpaid for primary care in the long run, will have to few primary care physicians and we fear that that is happening. the other type of problem is that if you overpay for certain services are likely to get more than. an example of that we believe would be around imaging services. where we think medicare has paid
7:03 am

too much. we've encouraged a lot of investment in imaging equipment to take advantage of that mispricing. once the equipment is in place, the profitability goes up dramatically. and you want to use that equipment more, more, more, because the marginal cost of using it is low. so you can have two types of ill effects. when his own supply of physicians, and one is on the type of services rendered. >> so could you elaborate on how we shift to a system that more accurately reflects the actual costs and how we may not have a federal policy that tens -- that tends to put things out of balance of? >> the physician fee schedule as instructed is focused on what are the costs involved in
7:04 am

providing a particular service. there are 7000 different services under the fee schedule, and relative values are established for each of these services. and the goal is to accurately measure the inputs and the costs that go into producing those services. we think there are errors in those measurements, and not small occasional ayers, but pretty broad errors in those measurements. so we've made a series of recommendations both to the congress and to the secretary about correcting those errors. the other lesser discussed challenge in the physician schedule is that it focuses only on measuring the input costs. in the market for all other goods and services in the country, price is not only reflect input costs, it reflects the value of the product.
7:05 am

and they also move to reflect imbalances in supply and demand. the construct of the medicare physician fee schedule pays no attention to the value of the service of the patient, nor to imbalance in supply and demand. the latter is why we have recommended, and congress has enacted, a primary-care bonus. it's a way of dealing with that value and supply part of the equation that fee schedule ignores. >> thank you. and thank you. i yield back. >> thank you, mr. chairman. mr. hackbarth, thank you very much for testifying today. i want to focus on home health agency issued if i can. first, i want to offer you a constituent case that we experienced a few years ago and get your reaction to that, and then also focus on a couple of the recommendations from a few years ago in this area. on the constituent matter, we
7:06 am

had a constituent who came to us after having three days of home health care, and the home health agency build $1500 for that care. it was submitted to the medicare program and the reimbursement back to the provider was actually double that, $3000. the reimbursement was double what was billed by the home health agency, an explanation for cms was we face a reimbursement on a 30 day episode care, based on the nature of the care over three days and 30 episode, that's what the reimbursement amount is. is that a particular issue you are aware of that we would pay, reimburse a provider double what was actually build? and if so, what would be a recommendation on how best to deal with that situation? >> actually, mr. gerlach, we exchanged some correspondence on this when it first came up a couple years ago. so in the home health area, and many of the other medicare payment systems, we pay on a per
7:07 am

episode basis. and do so recognizing some episodes will cost less, some will cost more, but those differences will tend to average out. the reason for paying on an episode basis is that it creates an incentive for effective management of the services. you eliminate the incentive to do more home health visits by paying on an episode basis. >> so in this instance paying double what was billed and sympathizes who to do what? wouldn't it incentivize providing more care because you will get reimburse more than what your actual, in essence, retail building would be for the service be? in some cases, the episode payment will be higher than the cost incurred, but in other cases it will be less than the cost incurred. and as i say, the idea --
7:08 am

>> over a spectrum of service you're saying? >> for all of the patients, home health agency cares for. some they will lose money, will lose money, some who make money and it will tend to average out. and the reason for using that approach is the great incentives do not provide more visits. a problem that we have in the home health -- >> wouldn't it make more sense now if a home health agency bills for $1500, that the formula for reimbursement ought to be the lesser of what that episode care was under the current formula? or whatever is built, whatever is less, wouldn't that make more sense? >> i suspect that over time what you would have is that all of the people who have fewer visits and episodes would start to gravitate up. we want to maximize the payment, and so we would just increase the number of visits until we get to the limit.
7:09 am

>> okay. >> so that's why medicare -- there's some very important issue on home health, and that is the payments are way too high on average. >> and that's really where i was going. back in march 2011, he recommends secretary should implement new authorities to suspend payment and enrollment of new providers if they indicate significant fraud. what's been the progress from your recommendation two years ago you can see from your physician, medpac, what progress has been made it seem as to address that problem? >> well, i can't provide a quantitative answer to that, but there has been fairly intense focus on fraud in home health in particular areas of the country like south florida. i think there's probably more of it needs to be done there but it is increasingly the focus of attention at hhs.
7:10 am

>> okay. then real quickly also recommended two years ago a per episode co-pay for home health episodes that are not pursued by hospitalization. what is that rationale for that recommendation? in particular for low income beneficiaries, and i visited a number of those types of homes the last few years, i can't foresee some of these individuals being able to provide any co-pay for the service they're getting in their home. what is the rationale and what you think the impact would be, co-pay was established particularly for co-pay individual? >> under our proposal, dually eligible beneficiaries would not be subject to the co-pay. so if we use that as the definition of low income, they would be protected. we think having a co-pay for all services is important in a fee-for-service insurance program like medicare.
7:11 am

that is one of the only tools that is available to manage costs. with regard to home health in particular, as you noted our recommendation focuses on what we refer to as admissions from the community. so these are not patient coming out of a hospital or skilled nursing facility. these are patients who are just admitted from the community. there are not clear clinical guidelines about when the community initiated home health service is necessary and appropriate. it's a gray area. some medical services, in fact in the last hearing, mr. mcdermott and i had an exchange about this, you know, you don't worry about the patients initiating demand when the service is something that's painful or risky. nobody wants to undergo that. but home health is different. there's no risk involved.
7:12 am

there is no inconvenience involved. in fact, it often lightens the burden on family members and friends. if it's a free service, you know, why not use it? so what we have recommended is quite a modest co-pay, like the $150 per admission, for the average home health episode that works out to about $8 a visit. which we think is an appropriate check for people to say is this really something that they need. >> very good. thank you mr. hackbarth. yield back the speed yield back the spent when i pointed to a second round but i like to recognize the ranking member for comment and question, and then dr. price was a final question. mr. mcdermott. >> thank you, mr. chairman. i just want to take a second to enter into the record, or ask unanimous consent o then into te record an article from the
7:13 am

"washington post" dated today that's called wanted to become a medicare costs, need to look at this chart first. it shows that hospital readmissions and medicare are dropping, and it shows that the percent of gdp over the next, future, if used what's going on the last few years it's going to stay level rather than continue to rise. i think you are familiar with these numbers. and i think numbers of the committee out to be aware of this particular article that shows that the aca is already having an effect before these things go into impact. before they went into impact last year. >> without objection. dr. price? >> thank you, mr. chairman. i appreciate indulgence the indulgence, just a few quick questions. this whole issue of post-acute care and the venue for care and the differential treatment, i think you mentioned that ought to be a clinical organization that ought to be making a
7:14 am

decision about the venue of treatment for patients. you wouldn't consider medpac a clinical organization? >> no, no. i'm referring to a provider. >> i just want to make the clipper can want to visit home health for just a second, because a lot of issues about overpayment in home health and the like. isn't it true though that if you look at the number of counties in this country and where the real challenges are, it's like 25 counties out of 3000 or something like that? >> yeah, so the patterns of home health use vary dramatically. in fact, the variation in home health is much greater than the variation in almost any other service. >> shouldn't we be looking at those targets? >> we should be looking at those areas in particular, but across the whole country we're still overpaying for home health
7:15 am

service. >> let me just touch on that if i may very briefly. both the margins you talked about, and i think that your margin analysis comes from methodology of -- [inaudible], right? >> no. this is her own methodology. >> what margins, refresh my memory on the margins that cheaply, the profit of margin they're making. >> for home health we are projecting for 2013, around 11, 12, 13%. >> are you familiar with a study, analysis 2013 study that uses financial reports filed with the sec that put the margins, and take into account significantly greater information than i think your methodology that put the margin at around 2.5, three? >> i am not familiar with that report. even mine the information that we are using is the information
7:16 am

supplied on cost reports by home health agencies. >> maybe we can follow-up on that, mr. chairman, and see if we can get more accurate data. this is a real concern because if we lower, the lowering of reimbursement for home health, then we may significantly adversely incentivize movement of those individuals into actually higher cost venues, and i think that's probably the last place we want. >> i would agree we don't want to do that, and i would be happy to follow in detail with you on this. we don't think that there is a risk of that by lowering the home health fee rate. >> thank you. thank you, dr. price. thank you for this hearing. there is a lot in this report to digest. i know there will be follow-up questions from members. we are 14 days to submit questions, and it should will be a number of them, including related to what are driving some of the lower costs, including
7:17 am

economy, shift into medicaid, the number of patients, issues like that. and i would ask if questions are submitted by the members, that you respond properly as you have in the past. with that the subcommittee is adjourned. [inaudible conversations] >> the head of the federal finance agency will testify on housing issues, including government mortgage financing by fannie mae and freddie mac. live coverage starts at 10 a.m. on c-span3. later in the days ahead of immigration and customs enforcement testifies about the recent release of more than 2000 illegal immigrants from detention centers. lastly john morton testified the releases were done for budgetary reasons. live coverage begins with the house judiciary committee at 1 p.m. eastern also on c-span3.
7:18 am

>> thirty-four years ago today, we began providing televised access to the everyday workings of congress and the federal government. the c-span networks created by america's cable companies in 1979 and brought to you as a public service by joerg television provider. >> next, former and current obama administration officials discussed the effect of new health care of new health care law can have on hiv/aids. the panel also looks at some of the challenges of implementing the law. the center for american progress hosted this hour and 20 minute event. >> good morning, everybody. my name is neera tanden and i'm the president of the center for american progress. thank you for joining us this morning for this important discussion of how health reform is addressing the needs of gay and transgender communities and people living with hiv.
7:19 am

reforming america's health care system is a massive undertaking. one of the president's advisers on health reform, i know that as we gear up for health care reform it will touch the lives of every american. that effort means it will touch the lives of the lesbian, gay and transgender community as welcome as those people living with hiv. the united states currently has 9 million -- 19 people living with hiv. hiv epidemic continues to raise and marginalize. like the uss russell, this topic is diverse. gay and transgender people live in all corners of our country and they come from families of all varieties.
7:20 am

regardless of the diversity of who they are, where they live, what their families look like, discrimination and marginalization remain common expenses for people with hiv and gay and transgender americans. despite advances in social acceptance and legal protections, gay and transgender people so frequently face discrimination in everyday life. in all aspects of their life. from education, employment and health care, to all of their social relationships. as a result it's harder for them to stay healthy, to get health care insurance coverage, and to get the health care they need. here at cap we are leveraging implementation of the affordable care act help eliminate barriers that keep the and transgender people in the with hiv from achieving the highest animal health care needs, health care that they need. in particular, our lgbt stated change project is working in states across the country to support better data collection,
7:21 am

better consumer protection, comprehensive and reliable insurance benefits, and a successful implementation of the medicaid expansion. when you look at the affordable care act, you know, those on the right complained that it is a bit of social engineering. and what it really is is trying to ensure that we cover all americans and provide them with good coverage. we should also look at the aca as an opportunity to expand basic rights for the lesbian, gay and transgendered community. all of these reforms have incredible potential to transform our health care system works for people, all people in the united states. but equally important is the fact that as we design a system that serves some of the most marginalized amongst us, we're helping to build a system that is better for all of us. and so as we see this opportunity for social change, i don't we recognize the importance of ensuring that all americans are covered. with that i'm now pleased to introduce our first presented this point, kellan baker.
7:22 am

kellan is the associate rector of capps lgbt research and communications project and he has been working on state exchanges. he's the mastermind behind all this work that we're doing here today, and with that, kellan. [applause] >> we here at cap agreed with vice president kind of health reform is still a big freaking deal. who our lgbt people? research shows that there are about 8 million americans, about 3.5% a population who identify as gay, lesbian or bisexual. about 700,000, according to the same research, identifies transgender. that means that at least 9 million americans identify as lesbian, gay, bisexual,
7:23 am
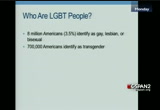
transgender. we know the from other research that many more people have engaged in same such a vehicle which becomes particularly important in the context of hiv/aids. and more than 25 million or more than 11% of the population acknowledge same-sex attraction. some of the social encumbrance about healthy lgbt people are able to be. unfortunately, predispose us to disparities in health status and health care access. some of the particular concerns the lgbt populist experience a lack of data, a lack of official data about what it's like to be an lgbt person in use today, last to me people in positions of power making decisions about our lives that believe if there isn't data there is no problem. a lack of relationship recognition. marriage equality is a health issue. marriage people are healthier on average, and if you're married you get the social support that
7:24 am

ensures you can be a part of the committee for your entire life. a lack of legal gender recognition for transgender people, it's not only appear to things like employment and health doing have an id document that doesn't show your true name or does it shall who you really are a it's also physically dangerous, particularly when transgender people encounter systems like the police or the criminal justice system. discrimination and violence that is both structural and physical, it gives lgbt people -- it keeps lgbt pull from taking advantage of educational opportunities, employment opportunities. it keeps us ask resignation from getting the health care and health insurance coverage that we need. provider attitudes, too often provider selected don't know who lgbt people are coming so they feel like a don't know how to
7:25 am

treat them appropriately. research shows that very little time is spent at medical institutions in the united states, medical training institutions to teach providers about how to recognize the lgbt people are among their patient populations and how to treat them appropriately. poverty, this is particularly true for lgbt people who are parents for women and for committees four-color. because of implement discrimination from lgbt people are still frequently the last hired and first fired. as result, they are up to four times as likely as the average american live in extreme poverty defined as nicolas and $10,000 a year. and homelessness, this is particularly true for lgbt young people been kicked out of their homes, which as we know roughly 40% of the out of home youth population in the united states is gay, lesbian, bisexual, transgender or queer.
7:26 am

as a result, lgbt people tend to get less insurance coverage. because of high cost of health care we get less health care and we don't have the coverage to help us pay for it. and as result we get diagnosed with conditions like breast cancer, depression and hiv more often. fortunately our girl is on it. secretary sebelius at the white house conference on lgbt health last year said the affordable care act may represent the strongest foundation we've ever created to begin closing lgbt health disparities. here at cap, as neera mention i run the exchange is project it was for this project in january of 2010 to take events of all the opportunities that the affordable care act provides us to start closing those disparities that keep lgbt. from achieving the highest attainable standard of health. we have for formal partners in 30 states with statement marketplaces that transgender law center in california, one in colorado, the lgbt record or
7:27 am
position in colorado. maryland health care for all, and they alliance in nevada. the project works not only in states with state-based exchange. also work year in d.c. on federal policy development. and we've in formal partnerships in many other states with both lgbt advocates and consumer health advocates. some of our national partners include community catalyst from whom you'll hear later from today, rural america, and raising women's voices. going to talk just briefly through the top five priorities in the affordable care act that our project works on the this is to provide us with background as we go into the panel discussion. data collection, this is number one pick your cab we see data clicking as the now because as we know if we can't expand with the problems are, it's hard to explain how we want them to be fixed. the affordable care act requires the department of health and human services to collect data on health disparities.
7:28 am
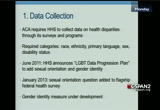
the required categories in the law our race, ethnicity, primary leverage, disability status and sex. but in june of 2011, sectors of announce an lgbt to progression plan that uses the authority of the affordable care act to collect data or to start collecting data on sexual orientation and gender identity. in january 2013, the national health interview survey, the federal government's flagship health survey added a sexual orientation question as part of this process. and gender identity measure is under development. nondiscrimination protection, the affordable care act extends the protections of federal civil rights law to the health care system for the first time. those protections include the ada, americans with disabilities act which was protections on the basis of hiv or aids steps to it also at the bottom includes title ix which has protections on the basis of sex.
7:29 am
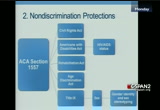
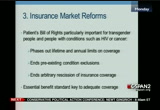
following the lead of equal employment opportunity equal employment opportunity commission, last year the department health and human services released guidance saying that they also interpret the sex protections of section 1557 to include gender identity and sex stereotyping. insurance market reforms, as neera mention an major combat of the affordable care act. many of the new protections in the insurance market are very important for marginalized consumers such as lgbt individuals. the patient's bill of rights for example, includes important protections for transgender people come for people with expensive conditions such as hiv or cancer. it phases out limits on coverage that were particularly problematic for people with expensive conditions. it ends presenting condition exclusions mean for people with hiv or transgender people won't be denied coverage on the basis of their previous medical history. and it is the practice insurance covers of arbitrarily rescinding coverage, especially when somebody gets sick.
7:30 am
the essential benefit standard which doctor kay's will talk about in more detail is also a major key for marginalized committees like lgbt folks when it comes to making sure that we get adequate coverage. prevention and wellness. we know that part of the reason that health are so expensive in the united states is because we are busy paying for the pound of cure rather than a ounce of prevention. the affordable care act puts its money where its mouth is about the importance of prevention and wellness. it creates e-15 billion dollars at the bottom, prevention and public health fund which supports new initiatives like the committee transformation grants program. that also makes certain preventive services free, including services that are particularly important for lgbt committees because of disparities we know we experience. including hiv and other testing, depressions green and tobacco use screen. that also builds community into the frame of health and all
7:31 am

policies, the national prevention strategy, specifically includes lgbt communities. and finally public and private coverage. related to the previous discussion of the insurance market reforms. the affordable care act will expand coverage to an estimated more than 30 million americans who currently do not have coverage. half of that will be through the expansion of the medicaid program come is the expansion goes through in all state. the new medicaid income eligibility rules will include many gay and transgender people who were present unable to qualify for medicaid coverage. the other 16-20 many people be able to purchase afford health insurance coverage through the marketplace. and importantly, the marketplaces may not discriminate no matter where they are or who is running them, on the basis of sexual orientation or enter identity. marketplace plans and other dh become the essential benefits based plans, cannot discriminate on the basis of sexual
7:32 am
orientation gender identity health condition or other factors. the marketplaces need to be able to engage diverse community, including lgbt communities. and the marketplaces may collect demographic data at the point of a global, which is particularly important for someone of our populations where we don't know the full extent of the disparities because we don't know enough about where our communities are, what their experiences have been and what their needs are. and with that, going to turn the podium over to doctor jennifer kates, to give us a rundown of the affordable care act and its effect on people living with hiv, or aids. doctor cates is vice president and director of global health and hiv policy at the kaiser family foundation. she is an expert on global health issues and is particularly known for her work analyzing donor government investments in global health, studying the u.s. government global health activities, and
7:33 am

tracking key trends in the hiv epidemic, an area she's been working in formal the 20th. she has served on numerous federal and private sector advisory committees including an institute of medicine committee commissioned by the white house to identify core indicators for assessing the impact of the national hiv/aids strategy and health reform law on hiv/aids care in the states, an important connection for us in our discussion today. dr. kates received her ph.d in health policy from george washington university, a masters degree in public affairs from princeton university's woodrow wilson school public and international affairs, and a masters degree in political science from the university of massachusetts. or bachelors degree is from dartmouth college. dr. kates, you -- your educated self, please take the podium. [applause] >> thank you. good morning, everyone.
7:34 am

we have been at kaiser family foundation analyzing and tracking the affordable care act for many different perspectives and hiv has been a core part of what we do. so to begin i just want to start off with this, because this was president obama on world aids day in 2011 getting a pretty historic speech about the possibility of ending the aids epidemic at some point in our lifetime. and for those of us have been working in hiv for very long time this was quite a moment and it's a moment of opportunity and optimism that i want to start with. the reason president obama made that statement and those of us working in the field are hopeful is that we have a combination now of new scientific advances with existing interventions that together is scaled up could begin to turn the tide on the epidemic. we also have a national hiv
7:35 am

strategy for the first time that the white house released a couple years ago which itself is the first copper is a strategy for the country and provides a roadmap for how the aca and other things can help get us there. however, have to move away from the optimism for a minute and look at the challenge. just a couple statistics but as kellan mentioned more than a million people living with hiv in the u.s., new infections in general have been stable in the u.s., which you could see as a good point of progress. they used to be very high and rising, but for the last decade they have been at the same level and we are not making a further impact. perhaps more on our way though, new infections are rising among gay and bisexual men who never visit the only group in the u.s. where new infections are rising. they represent 66% of new infections in the u.s. no matter how you slice it, the impact is quite alarming. people with hiv are more likely to be low income and uninsured than u.s. population overall and have a heavy reliance on
7:36 am

medicaid. most are not on treatment. yet as i was alluding to we have new scientific data that shows we can get to what many of us are calling aids-free generation, every skill of anti-retro viral treatment which is meant t of the note has madea huge difference in making people with hiv live much longer, much healthier, actually now has been shown to reduce the risk of hiv transmission to a negative partner by as much as 96%. that's very significant to the treatment has not just a clinical benefit but a public health benefit. but where are we in providing treatment in the united states it with hiv? this is something a bit of work and hiv you probably don't know this but if you do you see it all kind of fiscal the age of a treatment cascade and it's a very useful framework that many of us are using to understand how we are doing in reaching hiv, an aids-free generation. what you see to all the way to the right is that a quarter of people in the u.s. are virally suppressed. what does that mean?
7:37 am
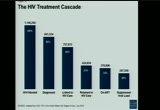
if you're virally suppressor have access to antiretroviral. that's when the risk of transmission and negative partner is significantly reduced. but as you can see from here, two-thirds of people with hiv are not even in regular care. not taking care and only a third our entry but it was a little hard to figure how we're going to steal a ticket to a three generation. this is one of the challenges. and opportunity is the affordable care act. some of the key provisions for people with a jvm and it is going to highlight a few that kellan also mentioned that are particularly important to people with hiv in these areas. there's many, many more. the first in a private workplace as we heard about, the end of the lifetime and angel coverage limits is important to people with hiv because the cost of care is so high. that has been a prohibitive factor in the past. the elimination of existing conditions exclusion which will go into effect for adults in 2014, again ever critical change
7:38 am
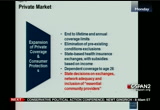
for people with hiv effectively if thei there stayed in the mart protections were not able to get insurance in the individual market until this took place to there are other new things every important for people with hiv, the state based exchanges with subsidies but the red part our flag in some areas where decisions are still being made are things are not yet clear what will actually happen. these decisions will affect people with hiv and affect lgbtq mideast states will do under exchanges to lead to network at a christian who to include in networks, what does it mean to us and to commend providers in those networks. this is part of the law. not stayed here but what with the benefits packages look like? essential health benefits company of the law which kellan mentioned is very critical because it has 10 categories of benefits that are now going to be required including prescription drug. very important people with hiv, it's the main part of hiv care, and up until this point is not
7:39 am
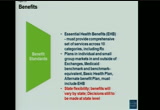
necessary included in many planes, or limits. all the new components will be required to some degree to have ehb stand. there's a lot of stay flexible in the benefits will still vary by state, which is how health care is today. i think it will be that some of the variation but in some ways that we a lot of variation and as many decisions to be made at the state level. medicare, i won't spend too much time on, there were two important things that happened with a lot of fixed challenges. the first was that as a 2011, aids drug assistance program cause, part of ryan white the pace for 80 drugs forget with hiv who are not eligible for medicaid, not on private insurance or have limits, when you on medicare and were in the doughnut hole, and needed to rely on that to pay this cost of
7:40 am

those costs would never count towards a catastrophic level. so is kind of a perpetual spiral in that place that need to rely on ryan white. that was eliminate with the law, and then that part the doughnut hole going into place for all people on medicare part d phasing out over time. medicaid's is perhaps the most important want to focus on. this is because already people with hiv rely heavily on medicaid, and we know many more are not eligible, have not been eligible for medicaid even though they are very poor. they key provision here was to change provision here was to change the grid any mandatory mandatory eligibility category that essentially said for all low-income individuals or nearly all in the u.s., if you are looking, approximate 15,000, for a single person or 15,500 for single person, that is the base for eligibility for medicaid. you know longer need to be a categorical eligibility, meet a categorical algebra. most of had to be very poor and
7:41 am

disabled. this changes since only a limited what we called a catch-22 for people with hiv which said, you are poor, give hiv, but you're not yet sick enough to qualify for medicaid. yet we have medications that not only can prevent you from getting sick but the federal government now recommends that anyone with hiv as soon as they get diagnosed consider going on antiretroviral treatment. so as a catch-22. you can't get this into your really sick but you get really sick because you can't get it. of the law actually changed that. as we all know the supreme court decision effectively made this a state option. it didn't take away the eligible to category but it allowed states to not expand and not be penalized for it. and what that means is to become the situation we have is that if you're a low income childless, nondisabled adult which many people with hiv are, particularly men, you are only eligible for what is considered for medicaid coverage in nine states.
7:42 am

and 26 h.r. not eligible at all. with the affordable care act is likely affordable care act is likely many more states are going to expand and i'll show you a map in a minute, but this is one of the big points of decisions that states are still making as well as on the benefit package for that expansion population. here's the map of where states are on medicaid -- decisions on medicaid expansion as of last week. this is statements like, executive statements or things that have moved. so it's not set in stone for all the states but as you can see, 27 have expressed support. seven are still weighing their options, and the rest of those can have said they oppose. when we look at this, what does this mean for people with hiv? on the good news side, but 60% of people with hiv have lived in the states that expressed support. however, most of the decisions are not final as you might've read in the news, florida, the governor came out in support the
7:43 am
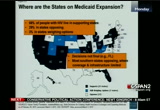
legislatures, is not in support and 11% people with hiv live in florida. also as you can see, most of the states in the south are opposing where coverage and infrastructure already quite limited. all those white states at the bottom on the states are opposing. that's a challenge. i want to turn to the ryan white program before the rabbit because even if all states were to expand medicaid, we know that insurance coverage alone does not equal access to care or receipt of care. this is why the ryan white program in this country ha has n so important its patient safety net for people with hiv. so for those who are uninsured or a nature can write what is been there there when it has had the resources to provide or fill the gaps in the care or complete their care. looking head with all the changes that are going into place with the aca, it's expected brian white will need to change but continued to be critical. what's challenge is that there's many unanswered questions right now to help inform how it needs
7:44 am

to change. without knowing which states are going to expand its a little hard to know how ryan white wanted to position itself. it's technically due to be reauthorize at the end of this you. what's the right time for the? but going for there's a lot of concerns of an integrated ryan white, expertise and providers into mainstream health care system and the networks can maintain the capacity the ryan white has helped build and bolstering the hiv workforce were there our projected shortages. and, of course, at the end of the day what we all hope for is any disruption, that there will not be any disruptions in care as people move into new coverage options are potential lives and your coverage option if income changes disrupting their care is not only very detrimental medically but as these applications for public health as i mentioned. so just to set up some thoughts for the panel, some key policy issues and challenges that affect or face both lgbtq me as most people with hiv within that community, what will be network, the network adequacy of all the new systems and the care
7:45 am

delivery systems that are put in place him the benefits of every key. outreach education and won't come we're at the point where we have to find ways to let people know about new coverage options, inform them of their choices and provide ways they can open role in new coverage where it is available. workforce entrant. scaling of the workforce is going to be key. the aca makes provisions for we still know there will be challenges. monitoring access in care, as people with hiv and as lgbt communities moving to new coverage options or are not able, how will the systems and extend the system are or are not working for them be assessed. medicaid expansion decision, health insurance exchange, and ultimately the future of ryan would. i will wrap up now and leave with some of these thoughts and look forward to you and what the panel has to say in the next phase. thank you. [applause]
7:46 am

>> thank you, for that thoughtful overview. we're going to move now to our panel discussion. our moderators morning is trafficking in the advisor lgbt policy and racial justice, and director of the fire initiative here at the cat. the fire initiative explores the impact of public policy on gay and transgender people of color. aisha. >> well, good morning, everyone. thank you, kellan, for providing that great interview -- overview for us. health reform includes the principle of universal design. so as we build the system does have some of the most marginalized among us can we're helping to build a system that works for all. i want to turn to the panel now to talk about what our committees need out of this effort and how we can achieve a single scholar and program director of the national hiv/aids initiative, at the
7:47 am

onion institute for national and global health law. he is a widely recognized expert on hiv and aids, and disability policy who served as director of the white house office of national aids policy. and senior advisor on disability policy for president barack obama from february 2009 through the summer 2011. in this capacity he led the element of the first domestic national hiv/aids strategy for the u.s. is also an alumnus of the peace corps program in swaziland and he received his master of public health, johns hopkins university school of hygiene and public health, and his bachelor of arts in chemistry from kalamazoo college. welcome. we also have my router is with us, the director public health policy and the office of health reform at the u.s. department of health and human services. where she oversees the cornea and then the invitation of the public health prevention and health care workforce policy provision in the affordable care act.
7:48 am

awesome. previously she served as a legislative assistant for the incident majority whip dick durbin from illinois. and as alleged a system for congresswoman hilda solis when she chaired the force for the hispanic caucus. she received her undergraduate education at the university of california at berkeley. we have kali lindsey with us as well, director of legislative and public affairs at the national minority aids council where he lives efforts to mobilize canaries of color around advocacy for the to hiv program at the national aids council, he is particularly focus on any the hiv epidemic for commuters of color and all this before so affected populations to the application of aca. and the national hiv/aids strategy. he completed his work in psychology and communications at eastern michigan university and began his hiv career in 2000 as
7:49 am

hiv prevention and testing counselor in detroit, michigan. shortly after learning of his own hiv diagnosis. and we have susan sherry with us. who is the deputy director at community catalyst, one of our partners, a national nonprofit advocacy organization working to build consumer participation in health care system. she has more than 25 years of experience in health policy and consumer advocacy and is responsible for developing and supervising community catalyst state based programs and issue camping work including health reform. she is also an instructor at the harvard school of public health where she teaches a course in community organizing it in 2004 and 2000 by shooting one of modern health care is 100 most powerful people in health care. she is a master's degree from goddard college and the dodgers agreed from massachusetts at amherst and she also put her doctoral coursework at brandeis university. and last but not least you already know kellan who is
7:50 am

associate director of the lgbt research and communications project here at cap. and kellan has a masters in public health, nasa public health and global public health policy and a master of arts in international development from george washington university. he received his undergraduate degree with high honors from swarthmore college. and i do believe that this is the most well educated and experienced them that i've ever had the budget to moderate. so thank you all for being here with us. we just learn from these presentations that discrimination, the travel along the fault lines of social and economic and inequality can system marginalizes lgbt people and people wer who are living wh hiv and aids. as a result, these populations expect severe disparities. thought want to turn to you first, jeff, and ask you to unpack this a little bit for us. can you talk to us about the other discriminatory social determinant of health like racism and violence against women and poverty?
7:51 am

and how they multiply disparities that we saw earlier? >> the first thing i would say is this is than the history of the epidemic from beginning. we saw this terrifying new epidemic come along, and the country respond with fear and also extreme discrimination target for gay people, people of color. the key populations that are currently impacted today are the key published over drug impacted from the beginning. so it's something that's been with us. i think, jim stopped on the treatment has to. she made us, if you work in hiv, it's your probably sick of it because we are all talking. that's what show some of these other factors how they're coming into play that people could have insurance coverage but if you don't have a doctor you trust of you can talk to, you are not coming for québec those types of things play out everywhere. we know that there's extensive research that shows that people more likely to adhere to hiv
7:52 am

treatment if they have a place to live. that might seem pretty self-evident but we can document this. so lack of affordable housing is a big barrier. there's still today we have the americas with this post act but people still face incredible amounts of state and commission. i have to say that i worked in hiv for longtime and when i was at the white house, either pros to work with mayra, one of the things that surprised me was the extent to which stigma discrimination is still so bad. i heard from people with hiv can we did these discussions across the country and i met privately with people, and people talking about the doctors engaging what they called occupational therapy. what they meant was medical doctors were afraid to get close to them. so they stood on the other side of the rim. that's happening today. so these types of things matter, but the reason i mentioned the treatment cascade, and jen didn't go into the details, but if you look at the casket, once
7:53 am

we get people retain into, the medical system does a good job of getting people on treatment in getting been suppressed. it's the front and where we lose 300,000 people, more than a quart of all people with hiv. after they been diagnosed and linked to care, mean that that one medical appointment with have not been retained into. so we need to think about maybe they didn't feel welcome, didn't feel like to talk about their health condition. so these types of things play out, and so did a good care for people with hiv, insurance coverage as a starting point and it's critically important but it's always of the fact that we need to address. having enough basics like food and housing and other things. and protecting people from discrimination a really important. >> so, trenton, one of the particular concerns of the lgbt communities, people living with hiv, people of color that the aca needs to address speak with some the initial concerns come from whether going to get access to cultural appropriate and
7:54 am

attempted health care services. one of the things that has been billed by the ryan white health care act over the past years is that we've really created institutions that have been welcomed into tenet and an environment where everybody else wanted to reduce us access to care. and you start having a conversation around that and where this would be disrupted in health care services or disruptions in providers. we also have to acknowledge the historical experiences of mistreatment and mistrust in commuters of color as well as lgbt communities have experienced discrimination from health care providers, and also just experienced discrimination just trying to get access to the system. so as we look at health care implementation is not just going to be about what the benefits look like but it's going to be about whether not the lgbt of americans are being overwhelmingly impacted by the hiv epidemic are going to have access to these services that they need. thing about the treatment cascade and one of the things we
7:55 am

know from recent analysis of the treatment cascade, by age and race is that younger americans are less likely experience -- less likely to engage in health care system. there's a story behind that don't have the necessary gotten to the heart of, but if a going to address health disparities we're going every chance in the epidemic, that has to be seated in a conversation around addressing hiv and infections among gay men who are the only there continuing to expensing increases. also have to conversation about how we spend access to transgender individuals who are traditional been locked out of the health of system and our ongoing impacted by the hiv epidemic. we can't just copy this. we also have to start answer the questions about once a get insurance access, whether going to get appropriate care? >> i think that poverty keeps coming up. i wonder if that's the question that we have an antigen.
7:56 am

like what does cultural competency me and what is the can build around ensuring that doctors and the system itself is transforming. how do we tackled that when we think about it? >> well, just a start i think a couple of those questions were kind of included in the early presentation. of this is about addressing the workforce but we talked about the medical system. while that's all going to be a long-term because of course those are health care providers that are going to the educational system right now, lisa is getting the conversation started about what kind of high quality education is going into the field and will be serving our community in every form health care in private. we also have to address the workforce that we're getting with right now. part of that is to continuing education and creating opportunities for our providers to understand the true facets and get really educated about things they can do right now in their own practices in an assignment where for any of us we have seen hiv specialty is someone else's job. many of our providers have
7:57 am

bounced them out the door and sent into the ryan white clinics because those are the institutions that rebuild the medical hall monitors. that's not necessarily going to lead to success in the future so we'll have to we prioritize and reprogram the current workforce to begin to take on some of the -- what they can do to do the in a way that is not going to displace the lgbt clients that they serve. >> policy decisions that offer really wonderful opportunities for intervention. so maryland consumer advocates have gotten involved in patient satisfaction and data collection is going to be for the health plans, new health plans in the changes in lgbt identity and information will be part of that. kellan mentioned david. that's a very concrete intervention point, state-by-state. or any state that is setting up its own exchange. decisions about exchanges, what
7:58 am

are the health plans that are going to contract with, what kind of providers and will be part of that? those are decisions being made now that are going to have huge implications for how this is going to play out. what kind of assistance programs are going to be available, help people navigate their decisions about what health plans they're in, when they go to change plans, what assistance will be available. will be lgbt community be part t of providing the system and helping people navigate, those are all things that are going to affect how it plays out and will also be concrete ways to monitor what happens. >> i also don't believe, we have had this two-pronged approach. the first of being looking at ryan white providers and the success that they have been come at the amazing model that they are as far as delivery to a patient by bush to have specific needs. ensuring that they are integrated into the future delivery system so that they are
7:59 am

connected with health insurance plans, that they may not that they may never been for me with in the past. network of providers. these are a lot of areas that traditional providers have not been estimate with the as a result of that, the department of the work of the health resources and services mr. risch as well as fda mrs. looking for opportunity to ensure that our providers are ready for 2014 and beyond. coupled with that, we looking at our existing network of providers like committee health centers and other providers across the country that are serving underserved communities and what can we do better to train these providers to better meet the needs of people living with hiv, and lgbt community. also agree specifically to meet the needs of the lgbt community. we have existing resources like the appropriate standard services standard, the class standards. we're about it at the department the time to update the standard. these are critical tools that
8:00 am

providers can have at the fingertips of the federal government can partner with to ensure that they are better prepared for the future. .. >> it's really about the experience of the health care system to date and why that hasn't been a success in many cases for people living with hiv and lgbt people and how the affordable care act has some of the tools to help us change that. because even going back, for example, to the discussionover cultural competency, there are so many instances in which
8:01 am

providers feel they don't know how to provide care for somebody with hiv. and frequently that means those people just don't get care. and we as a health system have traditionally not been as good, i think, as many of us would hope at addressing the experiences of people who are already marginalized, who are already having poor health outcomes even before they get through the door. and so talking about the affordable care act and the way it is looking at the his or to havic trends of -- historic trends of exclusion and saying we need to change that. we need to promote insurance benefits that mean people can get access to care, that actually come from providers who know, who have had training in how to treat them so that we're, as a system, moving from something that, frankly as we've already discussed, hasn't been serving our population so well that we're actually shifting to
8:02 am

incorporating the concerns in lgbt people, people living with hiv from the ground up as we're building these systems. >> [inaudible] just a little bit to talk about the accountability piece because i think it's probably a road that we're going to go down at some point in this conversation. but i also think the point for the hiv community is going to be the ongoing input into what the services look like that serve our community, and the reality with the ryan white program, institutionalized within the program was a community planning progress that actually gave the community authorization and a role about making decisions at the local level. those community planning groups don't have the same authority to the aca programs as they traditionally have to the ryan white program. so what is accountability going to look like? we talked about a lot of the discrimination protections and a lot of the health care expansion protections that are going to be built into the law, but implementation is where the devils are in the details.
8:03 am

are those programs actually going to look forward and not discriminate on our community, or are we going to have to be vigilant at the end of the day to set up kind of a monitoring role which has already been talked about through the conversation, but what does that look like, and what needs to be a place to make sure that the same control and ability to make sure that the programs and services work for people with hiv in the ryan white program are still going to be available in the aca-expanded programs. >> jen mentioned earlier many her presentation that there's clearly a lot of concern about what becomes of ryan white. we've known for a long time there's been medicaid covering folks, ryan white has been stepping in, and so the question i have for the panel is, well, how relevant is ryan white still? do we need the program, and what does the program look like as aca evolves? >> can i start? again, thinking about the treatment cascade and where
8:04 am

we're doing poorly, a lot of the areas we need to focus on are areas where ryan white traditionally has been almost the only people focused on that. getting people linked to care, retained. this is an incredible moment of opportunity. the fact that we're talking globally about the end of aids, let's hope we end aids in america first, and the way we're going to do that is when we get everybody in care, we lower incidents and all these things. we can look to the future, and we can look at massachusetts. they're a state that has expanded coverage, they expanded more than ten years ago their medicaid program, then in 2007 they got to near-universal coverage through broader reforms. they still have the ryan white program. we've seen they have lower incidents than other states. so i think that points us in a direction of how we can use the aca as a platform and build on
8:05 am

it with ryan white in smart, strategic ways. >> i'd also add that part of that effort requires -- in order to make the shift, you've got to get people enrolled in coverage. and, you know, the experience in massachusetts was that you can pass a law, but doesn't mean you -- but that doesn't mean you reach people. the populations we're talking about required special attention to doing outreach and actual enrollment which is going to require community-base withed lgbt organizations to be part of those, literally community by community outreach and enrollment efforts and to make sure people are given the support they need to get through those to see to the other end of actually getting the coverage. >> well, could you talk a little bit more about that? tell us what some state consumer health advocates have been doing
8:06 am

to incorporate the work into implementation? >> it's been an interesting process. there's a lot of state consumer health advocates who have been on the front lines of all ease issues -- all these issues. but now they're needing to develop and deepen their working relationships and build new relationships with a cross-section of community deep in their communities of a color, with lgbt organizations. and people need each other for this to work right. you need community-based organizations that are going to reach the populations we're talking about. those organizations aren't health care experts. they don't know the first thing about what a health insurance marketplace or exchange looks like, let alone what essential health benefits are or anything else. but the expertise is in the state consumer health advocacy community, and it's the partnership of the two that's required, and that was the experience in massachusetts as well. somebody needs to be at the
8:07 am

policy table saying these are some of the decisions -- take the ryan white experience and come to this table now to make that connection, to bring the experience. and similarly, the enrollment efforts are not going to be successful without really engaging in supporting the community-based organizations to participate in that. >> i couldn't agree more, and i really want to emphasize that building of awareness and engaging partners starts now. october is months away. that's when we go, that's when people can actually begin to enroll in plans, compare benefits, compare pricing and be able to find a plan that best meets their need. but right now is a time where we're reaching out to organizations to insure that they're aware of the benefits, that they're aware of what's coming down the pike and what's going to be growing in the future and will require their continued oversight. so right now you can go to health care.gov and sign up for current, up-to-date information
8:08 am

about the development of marketplaces across the country. but what we also understand is that a lot of people, they don't go to health care.gov. they're not aware of health web sites. so this is why hhs is critically focusing on partners and commitment-based organizations across the country where people are already going whether it's their or health center, their community center, whether it's their school. resources that are already at their disposal that if you can link to this information, we're in a better place to reach those hard to reach communities. we have a marketplace widget which is this i.t. term that you can put on your web site so people can click on that web site and immediately go to health care.gov with the relevant marketplace information. it is much more likely they will go to your web sites than ours. but for them to get the correct information about this opportunity is so important which is why we encourage you all to put that widget on your
8:09 am

web site. >> i would second that. not necessarily the i.t. piece because i'm not qualified -- [laughter] but just talking about the community organizations that are already out there and circling back, kali, to your point about accountability is there is so much advocacy out there among folks who have been working on hiv, among folks who have been doing the consumer health work. and i think part of the affordable care act implementation or the key piece for me is seeing how all of those threads are coming together. because there is so much that's already out there, but that's not necessary -- there's not necessarily the connections already made between, frequent, the consumer health advocates and the lgbt advocates. because frequently it's very difficult to talk sometimes about why health is an lgbt issue, why health is part of that movement for equality that so many people have been
8:10 am

participate anything. and the affordable care act, i think, really gives us a chance to talk about why the capacity of lgbt organizations to mobilize people and to talk about what's important in our lives can contribute to actually building, rebuilding a health system that is working for lgbt people, that's working for people living with hiv and is actually drawing on the resources of our communities to connect people with coverage, to connect them with information and to connect them with care. >> that, actually, takes us into an interesting kind of thought. you know, when you think about lgbt policy, priority issues and advocacy work, you don't really think of health care. >> i do. i do. [laughter] i stand alone, that's fine. >> marriage equality comes to top of mind. so can you talk to us about the connections there with marriage equality? i think it came up in one of the earlier presentations and health
8:11 am

care, and, you know, are the doma cases impacting that at all, do you think, in that outcome? >> i mean, marriaging is a health issue from a foundational perspective inasmuch as i mentioned earlier married people tend to be healthier. you have a caretaker in the home, you have social support, it's probably easier for you to get insurance coverage, to all of that translates to being healthier. so marriage equals health in many cases. but more broadly from the perspective of the lgbt movement is health is foundational. health is what comes fist. it's what you need in order to enjoy the benefits of marriage. it's what you need in order to be able to serve in the military. it's what you need in order to be able to go to work every day and take advantage of protections that we're all fighting for. so health is really the
8:12 am

underpinning, the ground on which so many of our other victories or our other goals are built. and so fighting for the ability of lgpt to be healthy, to protect themselves and their families and their communities is really, i think, as i said, the foundation upon which so much of our movement is built, and it's just that we don't always talk about it in that way. we don't always tease out the connections between employment nondiscrimination and insurance coverage or between serving in the military and the va, the veterans health administration, right? that's so important for so many veterans because you then have access to health care. and so teasing that out, the affordable care act, i think, is providing us and certainly me with what feels like an unprecedented opportunity to try to tease out some of those threads and say what actually is that connection between health
8:13 am

and employment, military, marriage. >> i would also add there's an economic security element of this especially for low income people or people who become low income real quickly as the result of medical debt. it's just, medical debt is devastating to whole segments of our society and also destabilizing to communities and low income communities too. so it's both help, but it's also -- health, but it's also the coverage aspect of this has economic security implications. >> so there's no doubt, clearly, that aca is going to be transformative for health care for all of us. but what's striking me is this undertone of fresh opportunity for coalition building and working across, perhaps, issue silos in a way to get people enrolled that we don't always do in the progressive community really effectively. so could you talk a little bit about what that's looking like in the state, working with religious leaders and others around this? >> it's been very exciting to
8:14 am

see the common ground in people getting out of their silos, and the first, one of the first state consumer advocacy organizations we approached was the maryland health care for all coalition. and a core part of their key leadership are faith-based leaders and faith-based communities and organizations. and we approached them literally when the marriage debate was happening in maryland. and they said, well, we can't necessarily agree to take on this project until we are sure our leadership can endorse us taking this on, and we have to, we have a process. we have a coalition process. and it was really interesting to watch. at the height of all the tension about the marriage equality debate, when they had a conversation and said these are the things that are happening to people, people are being denied health coverage, health status issues, the health care needs that are going unmet, the faith leaders just looked up and said, well, this has nothing to do
8:15 am

with the marriage equality debate, everybody has a right to have health care. of course we can take this project on. and that has just emboldened us to move forward, and that's been the experience in every other tate as we've moved forward to make the connection between the lgbt community and the consumer health advocacy at the state level. >> so how does the aca implementation and the national hiv/aids strategy kind of intersect? are there overlaps there? are they working tangentially? >> they most certainly are. one of the things we've been working on is trying to get a greater incorporation from the health care industry into the fight against hiv. many of our community-based organizations have been doing targeted testing on the side of health care clinics, and some of our communities have care clinics implementing routine testing, but an each -- an even greater number of people have
8:16 am

been seeking care at ryan white facilities. those individuals are interacting with the care system that's somewhat removed from the rest of the health care system, and the aca gives us a unique opportunity to really ally the ryan white system with a lot of the health care system that's available to rest of the country. and more importantly, particularly in the context of dealing with the hiv end epidemc among young gay men, it really gives us a an opportunity to work with both partners in the relationship. traditionally we haven't opinion opinion -- we haven't been able to work with the negative partner. but now we recognize that with treatment and prevention which is a scientific development, we can reduce the likelihood that they'll pass that infection to their partner, it's a new opportunity for us to engage pote of those individuals. and -- pote of those individuals -- both of those
8:17 am

individuals. but even more promising to me from the aca and the ryan white combination is the fact that it allows us to mobilize the system of whole health for people living with hiv. one of the misnomers that we've always responded to hiv first because it's infections. it's chronic, and it's the one that scares people the most. but the reality is that many people living with hiv are living longer. they're dealing with a series of chronic conditions, and not all of their needs can be met particularly when someone requires specialty care. the aca creates a pathway for us to be able to provide comprehensive health that not only includes their health profile, but also the health of their loved ones. >> could i just add, the strategy where one of the three goals was to increase access to care and reduce hawaii-related -- hiv-related
8:18 am

disparity, one of the step is the to immediately link people to continuous, coordinated, quality care. so the aca is really the base for achieving that critical goal and that action step. >> i think that's another sort of just going back to the role of the affordable care act in drawing a lot of these threads together because i think we see it on a couple of different levels. we see how it's drawing the community organizations together in this transformation of a system that's going to happen sort of whether or not we're paying attention and is going to happen much better when we're all engaged and aware. it's also happenings in the sense of all of the work that the administration has been doing, i think, over the last couple of years more generally about health equity, about health justice broadly and how lgbt folks, how people living with hiv, how we're all part of that system. it's not hiv over here and lgbt
8:19 am

over here and ordinary people with cardiovascular disease somewhere behind us. it's all of us contributing to a system that is making things better for everyone because it's recognizing the ways in which the social determinants are so interconnected for our communities and how if we're addressing the needs of folks living with hiv or the needs of lgbt people as part of a broader focus on prevention, healthy people, health equity that we're actually creating this much stronger foundation from moving the conversation forward and the country as a whole about why the u.s. health care system exists and how it is supposed to serve all of our different communities and all of our diverse folks coming from all kinds of backgrounds. >> may -- mayra, could you talk about -- [inaudible] >> i couldn't agree more.
8:20 am

every major topic that we're faced with on a day-to-day basis. on a national level we often here elected officials talk about creating jobs and building better schools and building stronger communities. health is connected to every single one of those goals. on an individual level, health, it's fundamental to opportunity. if you're not, if you're not -- if you're sick, if you can't access the services that you need, your opportunity is stifled. and disproportionately communities of color, lgbt communities, our opportunity has been stifled because of the health disparities that have been persistent in our communities for generations. the affordable care act helps break that and really, you could argue s the biggest piece of legislation our country has ever seen to target health disparities. it's incredibly exciting. when we're talking about prevention, this isn't in 2014 and beyond, it's right now. 71 million people with private insurance today have access to preventive services without cost-sharing requirements.
8:21 am

and that might not seem like a big deal to people, but even people with private insurance, that $40 co-pay or $20 co-pay, they're thinking about $40 for their gas or groceries. >> it's a big deal to me. when i went to the doctor, i went to the gynecologist and i was like, oh, i actually get to come and get my annual care? it never occurred the me it was aca. >> that's what's so great about it, you're able to translate policy into real action for families today and be able to talk to people on a normal basis what we're doing to change the health care system the to better meet the needs of our communities. >> well, so let's talk about, um, enrollment. people need to be covered. it sounds like the big benchmark that's coming up later on this year. so i'll just throw it out there to all of you, what can we be doing to make sure that the vulnerable populations are involved in the big effort, kind of the big push to make sure
8:22 am

they're covered, and what else can we be doing on the ground to help in. >> i can start. today at 2 p.m -- [laughter] there's the first national stakeholder call run by the department of health and human services where it is completely open to everyone who's interested in hearing about these efforts and what's coming down the pike. we strongly encourage everyone to participate as part of that call. i'm sure many of my panelists will be part of that discussion. and i think moving forward identifying those opportunities to become better informed about the marketplaces. one major opportunity that the department will be releasing very soon is the-and-a-half gater program. in state-based marketplaces as well as partnership marketplaces, the navigator program will exist to be that link between communities and the marketplace, to enroll people in the -- go through the application process to better understand what health insurance plans are being sold, what the cost is, how to compare the invests provided, to have a better understanding of what's at stake and how it can best
8:23 am

meet your needs. that's one opportunity. other than that the department is also providing training opportunities to engage with our partners to better understand the process. a train the trainer approach. the federal government's not going to be able to reach everybody, but we know that through the work that we've been able to do with medicaid enrollment and medicare part d, we have valuable lessons to learn to reach these hard to reach communities. how can we apply those lessons learned not only on the national level but also regional bases. regional correcters will -- directors will start to have conversations. obviously, needs are different in every corner of the state and how can we best meet those needs. >> i think the general message is we're here to recruit you, everyone, to get involved. because it's actually, we know not just about lgbt folks or people living with hiv, more
8:24 am

than three-quarters of people who are going to benefit the most from the affordable care act who are going to get enhance ad insurance benefits, maybe access for the first time, don't actually know anything about the law. and that's so true for so many of our communities who have been so dissociated from the health care system or disenfranchised from it. so i think we're really here to recruit. [laughter] >> and i would add a lot of this work is going to happen at the state level. it's certainly for states who do state-based exchanges, for sure -- >> are there differences between the states -- >> yes. >> okay. >> jump in. >> one of the differences in the states running their own exchange, you know, there's a state table, and you're dealing directly with your state government. so, for instance, the state in has just put out the call for proposals for navigators. and advocates, we're all working with the state consumer advocates, lgbt community groups are all, like, learning about that and are making decisions
8:25 am

about should they put in for that, reference their own capacity and connections. at the federal level -- and the decisions just stay there. b about to 30 states will be doing either a partnership or have a federally-facilitated exchange whoo -- which means there's a two-step process. the state health advocates because people are planning together to say, okay, what does our state need, but then needs to be communicating directly with the federal government. and hooking in with the types of connections that mayra's describing. and that'll be a federal grant process for the navigator programs. and i think, you know, this would probably be less resources proportionately than in the state-based exchanges. so this additional work that will need to happen, um, at the
8:26 am

state level even for the federal exchanges advocates, i think, are going to be trying to coordinate tables together where everybody comes in and discusses how do we do media efforts, how do we do coordinated efforts, how do we do, um, the social media in order to reach the populations to supplement what would be the federal effort. >> could i just add? >> yeah. >> there's so much negative energy for opponents of the aca. one of the things we needed was talk up the benefits because not everybody knows it's a good thing. some people might think they should wait. we want people to sign up right away. and talking to community-based organizations, there are a lot of federal resources, but there will not be a perfect plan handed to you on a silver platter. don't wait. this is an opportunity for our community. you need to do what you can in your own community, seek out these resources, but don't wait until it comes to you. you need to go to it. >> and definitely from the
8:27 am

perspective of the national minority -- [inaudible] we represent over 3,000 community-based organizations throughout the country, and one of the things that we're trying to do is pass along a lot of the information that's being put out by hhs because it's already been well articulated that the cbos have a traditional role in helping the people that they serve get access to these expanded programs, and we need to put the tools at their fingertips. so the council really sees itself as playing a translational role, taking that information from the federal government and putting it at the fingertips of the people at the local level. but in addition to that, we coordinate the united states conference on aids every year, and we bring in about 2500 to 3000 health care advisers less than 30 days before the aca programs begin enrollment, we're going to be ready to get all your folks. so you can leave new orleans on september 11th -- funny date, right? [laughter] you can leave new orleans on september 11th, you can go home
8:28 am

and start enrolling people in the aca programs. >> well, great. we've got so much good information here. i know you all want to ask questions, so we're going to open it up for questions for our panelists and also for jen. if you have any questions about the presentation you heard earlier too. right here in the back. >> thanks for a really optimistic panel. it was wonderful to hear. my name's josh, and i'm with the national assembly on school-based health care. i really heard a lot that i liked about understanding that insurance is not access, you know, understanding accessible is important, i think it's something school-based centers do well. i'd sort of like to ask the rest of the panel how you could see schools intervening in the cascade that we saw, how we could prevent kids from being
8:29 am

part of that graph in the first place. >> so one of the hats that i used to wear that i don't wear too much anywhere is i used to sit on a board called the education council of the united states. i'm glad i got it out. and essentially, what they've been looking at over the past two years is how we create more expanded access to sex education both in the schools as well as in community-based settings for individuals that interact with their health education or with their public education in a variety of means. and the reality is that we still have a lot of work to do because the fight on how comprehensive sex ed gets implemented is at the local level in many of the same way it is aca fight is going to be. but it has to be married with access to those school-based health clinics that are authorized by the affordable care act, and there has to be a marrying between the services and types of programs that are available that are also be instruct inside an age-appropriate and
8:30 am

comprehensive manner. and if we're marrying the two with the resources by the aca and really mobilizing things like the real act which are trying to put, you know, legislation forward to actually advance access to comprehensive sex education, then those, i think, are some of the strategies that we can kind of marry the aca expansion efforts with the other tangential and, you know, cooperative efforts to expand access to the -- [inaudible] of sex ed as well. >> i think one of the other things that the school-based health centers really represent for me is there's so much that happens outside of the doctor's office, outside of the interaction with the provider, and that's so clear in schools, right? we know what happens with young people in schools who are bullied or made to feel like they don't belong, and i feel like school-based health centers and other federally-qualified centers, other kinds of clinics that look more broadly than just the clinical services to actually talk about what are the circumstances that young people or lgbt people or people with
8:31 am

hiv are living in every day and how are those affecting their health, i think that's really a pretty key nexus as well. >> yep. right here. >> hi, my name's -- [inaudible] murphy, i'm with metropolitan community churches. i have a question about undocumented workers. ryan white is such a critical pillar in how services are delivered to people who are undocumented, and the vision that you've crafted or that you're articulating for how implementation would go doesn't necessarily speak to the barriers that this population will face. it's a highly vulnerable, very much at-risk population, and commitment providers are in-- community providers are continually dealing with large increases among undocumented. so i'd like just a comment from any of the panelists about what's the vision for care and where ryan white fits into all of that.
8:32 am

>> you know, if i could start i would say, you know, that's one of the key reasons why we need ryan white going forward. first off, we're going to need ryan white for people who have insurance, and 70% of clients today have insurance, so it shows you it's not doing everything we need, so we need ryan white to wrap around. but also for the undocks yuled, they're -- undocumented, they're not eligible for aca coverage, so we need to make sure we have the ryan white program to serve these communities. but also as we talked about earlier, ryan white has provided effective services to immigrants, and we need to make sure that we retain that a expertise. >> there's a provision of the aca that is also going to be relevant to undocumented folks which ising -- and it's hospital, nonprofit hospital community benefit requirements are going to be very important to undocumented populationings as are, as is the fact that hospitals now have to report and
8:33 am

document what their charity care policies and financial assistance policies are to the irs. those are going to be very important tools because in massachusetts charity care, financial assistance remains one element for populations that were not covered, and that's going to be true going forward until we deal with the immigration issue. >> and also -- sorry. >> no, go ahead. >> and i also want to make sure we keep our eye on the conversation going forward. there's also a mechanism to be able to address some of the shortcomings that we didn't get to expand access to immigrants through the aca to try to correct some of those wrongs in immigration reform. >> the undocumented part of our commitments, they're part of the -- communities, they go to school with our children, they work with us. and i think first and foremost the administration is committed to passing comprehensive immigration reform, and i think that is, like you said, one of those issues that's outside of
8:34 am

the clinical setting and will impact the health of these communities in ways that health insurance probably be won't even touch. so let's keep our eye on the prize and better identify the needs of these communities moving forward. >> in the front there was a question. do you still -- okay. right there in the back. >> hi, my name's alyssa, i'm with doctors for america. i was just wondering what kind of resources are available for providers who are looking to become more aware of lgbt health issues and be more trained on it and be more culturally sensitive on the issues. are there any programs out there for providers specifically? >> yeah. there's a variety. substance abuse and mental health services association has a wealth of resources specifically targeting providers to better serve the need of lgbt
8:35 am

communities. particularly assisting community health center efforts. we are reevaluating, like i said, our class standards which is culturally appropriate services standards for care, there's been a number of discussions across the country with lgbt advocates to better address their needs in the provider education materials that the department has available. that's forthcoming, but i do think that this is a conversation that is ongoing and the partners here on this panel actually have resources available to also assist. >> yeah, there are definitely many community organizations that in many cases have partnered, for example, with the federal government. the national health service corps has tripled in size, and hhs has been very interested in making sure that those young, starting-out providers have the opportunity to get competency training. and as i said, there are many trainers who do that in various parts of the country.
8:36 am

another major resource is actually the joint commission. my parents are health care providers, so i know all about, you know, there's sometimes a little bit of a tension between the standards that are set out and how providers feel like they're actually equipped to meet those standards. so when the joint commission established its new standards that include nondiscrimination on the basis of sexual orientation and jebder identity, they also started a project to make materials more widely available so clinicians actually felt they had the tools to make that change. so there's a monograph from the joint commission, and that pulls together resources mayra has mentioned from the federal government and others. >> yes. question in the front. >> hi, i'm david, i work with whitman walker health. and i'm happy to say that we're often the anti-cascade remedy. you know, we do terrific work in
8:37 am

the community, the hiv community, lgbt community. we're moving toward being a patient-centered medical home. huge expense. no money out there to help us get there. we have issues where community-based organizations that have sound business models suffer at the hands of one organization or one entity changing a policy. on one medication we went from a reimbursement model to a replenishment model, and it's taken almost $900,000 out of our operating budget in two days. who is out there working across agencies saying, you know, as we move towards aca when everybody has to compete on quality, you can't disrupt these business models and expect people to not be impacted all the way through the care continuum.
8:38 am

>> you raise a very good point, and i think one to have realities that we know about the affordable care act is that everything's not going to be perfect when it's implemented on day one. and one of the things that didn't get mentioned when we were talking about my bio, i actually came from a federally-qualified health care center and understand that the transitional processes are quite expensive, they're quite laborious. but at the end of the day, they actually do provide better patient care to the individuals that you're serving. but i can't give you a panacea answer that's saying all of us or any one entity is out there looking at any of these discreet variables and figuring out how to activate each one of those. i think we can try to mitigate some of those consequences at the end of the day. this is a new, um, challenge that i'm just learning about by your articulation, but if you want to talk afterward, i'd love to try to find some ways to
8:39 am

address it. >> yeah. i would also say, you know, i don't have a good answer, and i'm not dismissing you, but i think we know it's going to be messy. there's going to be things that come up that are unanticipated. i also think that's why people need to be engaged. whitman walker health, i encourage you to do more on the policy front because a lot of these new stakeholders that are coming to play may not know everything they need to know. so we all need to make sure we're doing as much as we can to educate people about towards of hiv care, implications of different policy choices they make. but if we do everything we can possibly think of, it's still going to be a messy transition, but we'll end up in a were the place. >> -- in a better place. >> it's definitely not a bandwidth issue to take lightly either for organizations or community members themselves. but it really, i think, does go back to the issue that the rules as we know them are being rewritten right now. and if we are not involved as community members, as organizations that are affected, as groups that are providing care, then we are going to be
8:40 am

left out in too many cases. and with regard especially speaking from the lgbt per spect pif, it's not malice, right? it's just there are so many moving pieces that making sure the pieces that need to be there, the folks who need to be around the table are there so that our voices are heard as these policies are being crafted and the decisions are being made. >> i think that's a great charge to end with. >> i had another example of where that same problem has arisen around different systems not necessarily interacting with each other, and it was the example of california which moved early to expand coverage. and there were some unanticipated consequences not because of malice, because the state agency, the ryan white folks were not talking. and so there was assumptions about what would happen to people with hiv. fortunately, that was caught, and the communities came together and were able to mitigate it and now the rest of the country is learning from that experience. but this is happening as we go, so sharing this information --
8:41 am

and we often look to whitman walker health as a model to what asos can do. so part of it is getting your story out there. >> and one of the things that cel land is going to continue to do, i think you might have all grabbed the one-pager outside, there'll be a report coming out, is it next month in april? early next month it's going to talk about all these issues, and as you guys have ideas, thoughts or questions that surface and bubble around how this is going to be implemented, bring them to us pause that's -- because that's exactly the work kellan is doing, what can we do to resolve some of the kinks that perhaps folks aren't thinking about. so thank you very much for coming out, and thank you to our awesome panel. please, continue the conversation. and they'll be here if you guys want to talk to them before you go. [applause] >> the head of the federal housing finance agency, edward
8:42 am

demarco, will testify on finance issues at 10 a.m. this morning on c-span3. and later, the recent release of more than 2,000 illegal immigrants from detention center. last week john morton testified the releases were done for budgetary reasons. live coverage at 1 p.m. eastern also on c-span3. >> 34 years ago today we began providing televised access to the everyday workings of congress and the federal government. the c-span networks, created by america's cable companies in 1979 and brought to you as a public service by your television provider. >> michele bachmann, wisconsin governor scott walker and newt gingrich spoke last week at the conservative political action conference known as cpac.
8:43 am

we'll also hear from congressman steve king of iowa. this is an hour, 15 minutes. >> five to six years ago the national debt was not really a big deal. people didn't even know we had a national debt or deficit. but then a grassroots movement known as the tea party started to emerge. [cheers and applause] and what made the tea party so effective was not only it came from the grassroots, but it had three core values; fiscal responsibility, constitutionally-limited government and free markets. and because of the tea party, we were able to put patriots like michele bachmann, joe walsh into congress so they can make sure that congress will not continue to spend my generation's money. [applause] we need to save the tea party so that we can save america. [applause] ladies and gentlemen, please
8:44 am

welcome jenny martin from the tea party patriots. [cheers and applause] ♪ >> thank you. [cheers and applause] picture this: college students in this country who are optimistic about the future and look forward to living the american dream. after college they pursue their careers and begin to make a living. they become parents and put food on the table for their children, save for their retirement and still have money left for leisure activities and vacations. as they become senior citizens, they mow their retirement is secure, backed by a strong, sound dollar.
8:45 am

their health care needs are met with the best quality health care on the planet, and they are at peace knowing their life's accomplishments will be passed on to their children and grandchildren. imagine our country as the most charitable country on earth and those who are unable to take care of themselves, are uninsured or have hit hard times due to unemployment benefit from america's charitable, generous, giving spirit. visualize a future where the economy is growing at a steady pace. entrepreneurs are building businesses, taking risks, innovating, investing, employing millions of americans and as they employ these americans, they move them up the economic ladder.
8:46 am

this growth leads to a balanced budget, and our nation has a surplus. we're able to pay down our debt. citizens know that growth and opportunity abound. they are confident. they are proud of their country. this is the vision tea party patriots have for america's future. [applause] a constitutionally-limited, fiscally-responsible government where free markets thrive. [applause] and for this vision we've been mocked, marginalized and maligned by president obama, nancy pelosi and speaker -- and majority leader reid.
8:47 am

and people from the republican establishment like senators john mccain and lindsey graham. they are contemptuous of our vision, and our vision is distinctly different from today's reality. our country is $17 trillion in debt, and we're headed to bankruptcy. last quarter our gross domestic product shrunk, and wall street profited. seven of the ten wealthiest counties in america are right here in boomtown d.c. it's very much like capital one -- the capitol in district one in the hunger games. standard operating procedure.
8:48 am

yet in the heartland, unemployment is in the double digits. homeowners are trapped, unable to move to better opportunity. when obamacare is fully enacted, eight million people will lose their current health insurance. 30 million people will still be uninsured. and a family of four will have to pay $20,000 a year for the cheapest health care plan. studies show that medicaid surgical patients today are far more likely to die than those who have no insurance at all. the affordable care act is a con. in reality it's unaffordable, callous and cruel. [applause]
8:49 am

our country's equivalent to the hunger games tribute will be the patients who die under this law. [applause] most of our elected officials do not know how to even solve the problems facing our country today. the establishment are content to attend cocktail parties, clinking glasses toasting one another while we suffer. the contrast is clear. is this the america you want? >> no! >> do you want representatives who sit back clipging glasses -- clinking glasses, lining their friends' pockets on k street and wall street? >> no! >> or do you also foresee a better future? >> yes! [applause]
8:50 am

>> do you want fighters who will stand on principle defending our freedom? [applause] our constitution is worth fighting for because freedom is worth fighting for! [cheers and applause] and our principles, our principles are worth fighting for because our principles will be a better future for all americans. [cheers and applause] tea party patriots wanted principles fighters. at cpac 32 years ago ronald reagan attributed his victory to a set of principles, principles which were protected and nourished by a few unselfish americans through many grim and heartbreaking defeats. the reality today is grim and
8:51 am

heartbreaking. we have so many reasons to be encouraged because we have unselfish americans around this country who are protecting and nourishing our principles. [applause] examples, examples like senator rand paul -- [cheers and applause] congressman louie gohmert. [cheers and applause] and a few steadfast, stalwart, principled fighters on capitol hill. and we have unselfish americans around this country. examples like our warriors in wisconsin who have been on the front lines fighting -- [inaudible] [applause] examples like michael -- [inaudible] jo ann terry -- [inaudible] who helped coordinate our
8:52 am

efforts to defend representative democracy in their state as governor scott walker stood and acted on principle. [cheers and applause] one patriot stood at a town hall and challenged president obama questioning his demonization of the tea party. it's no surprise that this principled fighter, ryan rhodes, is from iowa. [applause] there's another iowan, congressman steve king -- [applause] who challenges president obama and nancy pelosi on capitol hill and defends the tea party. and for this karl rove threatened to primary him. >> boo! >> tea party patriots gave cindy pew the nickname sunshine cindy
8:53 am

because she is one of the most cheerful, happy patriots we know. congresswoman michele bachmann inspires -- [cheers and applause] this mother of two to stand on principle and run for elected office. today cindy is a state representative in minnesota. [applause] wayne hertzog organized a coalition in the unlikely deep blue state of washington. they went door to door talking about taxes and government spending, and they flipped their state senate to a fiscally-responsible majority caucus. [cheers and applause] willing the torch of liberty, the constitution in our country
8:54 am

perish or endure? if we stand and speak for our principles, if we show americans our vision for the future, if we fight for freedom, our country will endure. [cheers and applause] will you clink glasses with the powerful elite? >> no! >> will you link in the face of opposition -- blink in the face of opposition? >> no! >> or will you stand up and fight boldly on principle? >> yes! [cheers and applause] >> patriots, stand with us and fight for freedom! [cheers and applause] fight for our constitution! fight with us for the rights endowed by our creator; life, liberty and the pursuit of happiness! fight for a better future like ronald reagan did!
8:55 am

[cheers and applause] like rand paul, michele bachmann, steve king, scott walker, like tea party patriots do around this country every day! [cheers and applause] and when you stand and fight, we will stand with you! when they -- [inaudible] on capitol hill, together we will are their backs. concern we will have their backs. we will stand and fight for those who fight with us! [cheers and applause] liberty will endure! and our country will flourish as a result. take up a torch, fight for freedom, fight for a better future. fight! [cheers and applause] thank you so much. god bless you. god bless america. [cheers and applause] ♪
8:56 am

♪ the constant theme of this conference has been talking about the debt, talking about how conservatives can rein in the spending so my generation can prosper. but when i look at washington, i don't think the problem is that there's too much partisanship, there's too much bipartisanship. both parties are agreeing to equally mortgage my future away. they're agreeing that it's okay to spend a trillion dollars we don't have. but there is a caucus of people that have stood up against republicans and democrats so that my generation does not have to inherit trillions and trillions of dollars in debt. one of those people is congressman steven king from iowa. >> iowa! [cheers and applause] >> someone who has stood up for constitutionally-limited government, fiscal responsibility and has the courage to call a republican a rhino and a democrat a liberal. ladies and gentlemen, please
8:57 am

welcome congressman steven king from iowa. [cheers and applause] ♪ ♪ b. [cheers and applause] >> thank you, good morning! good morning, cpac! [laughter] you know, i walk in this building a couple of days ago, and people come up and say thanks for giving me some energy and inspiration. what are you talking about? i'm the one that draws the energy and the inspiration from all of you. and when i go out of here, i'm going to go out of here like a rocket to engage those people that are upside mining the pillars of american exceptionalism. [applause] some more. but i have some thoughts that i wanted to start out with, and that is that about three weeks ago -- i'm on an exchange program where we negotiate with the european union, and i go there every other year, they come here in between. i was sitting in a conference, and they had an expert on the
8:58 am

middle easts there, and he began to talk to us about how the muslim brother hood and the arab spring that had taken place and summer and fall and maybe another spring, that arab spring and that muslim brotherhood, according to him, is a hollow ideology. a hollow ideology. and they're willing to die for what they believe in, and i listened to that, and i thought i've gone to church here in western europe, and they are museums if americans don't go over there. they're museums every day but sunday at least. and where is the hollow ideology? i listened to one of those elected representatives say to us that he add inadvertently outed himself as a christian and, therefore, everyone suspected his policy agenda as being rooted in his christian beliefs, and he couldn't be effective as a legislator. not in america. we're the exact opposite. if people don't understand that we have a core faith of beliefs, we don't trust their agenda.
8:59 am

and that's the difference. but i'm watching it come pack here here to the united states, and i look at the agenda coming out of congress recently, and it seems to me to be a hollow agenda. there's a lot more to this country than buy, sell, trade, make, gain. yes, economics are important and, yes, free enterprise capitalism is a pillar, but it isn't the sole point, and it isn't the only picture, the only piece of the picture of the shining city on the hill. [applause] there are some people within our movement that want to rebrand the republican party. now, they're never going to rebrand us conservatives. [applause] the things that we believe in we've believed in for generations and, in fact, centuries. the founding fathers understood this. they saw that vision from god
87 Views
IN COLLECTIONS
CSPAN2 Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
